
Section 1: Introduction
Self-funding has become one of the most widely used forms of risk financing for employee healthcare coverage. In 2000, about 48% of all employers self-funded their employees' healthcare coverage. Five years later, the percentage of self-insured employers had grown to the mid-50's, and in 2015, fueled by the Affordable Care Act (ACA), the percentage of self-insured employers had eclipsed the 60% threshold and is expected to continue growing at a significant pace.
At the present time, more than 80 million individuals – 60% of all >workers under the age of 65 – are covered by self-insured employer health plans. Given the rising cost of healthcare, and the complexities associated with ACA compliance, more employers will be likely to explore self-funding as an option to lower or offset the cost of healthcare delivery to their employees. With such sustained growth, the strategic use of stop loss captives, to augment traditional self-funding, is also likely to grow.
Medical stop loss captives have enjoyed niche-level popularity for several years. However, during the past few years, their acceptance has risen to a more mainstream level. Increasing familiarity with alternative financing options, coupled with increasing ACA regulatory discomfort, are probably responsible for this rise in the comfort level employers now feel with regard to stop loss captives.
As a result, the same alternative-risk financing techniques that, for decades, were used to reduce the cost of casualty risks, have recently found a new degree of popularity within self-funded healthcare programs.
Section 2: What are the benefits in arranging medical stop loss cover(age) through a captive?
The first, and most obvious, benefit is reducing and stabilizing the overall cost of providing healthcare insurance to employees on a long-term basis. The premise any alternative risk structure is based upon, is that of achieving the most appropriate balance between risk assumption and risk transfer – in order to optimize savings, while at the same time supporting the organization's risk management, financial, and business objectives. Captive participation in excess coverage (Medical Stop Loss) that supports a self-insured plan, will amplify the benefits derived from self-funding alone. For smaller employers, participation in a group captive can provide increased access to many of the same advantages (increased risk spread, service provider cost leveraging, surplus dividend sharing, and so forth) that are enjoyed by larger organizations with a single-parent captive.
Since the underwriting variables for each employer and captive are different, it is difficult to provide potential cost savings figures. The primary objective of a properly structured alternative risk program is to distance the employer from dependence on more volatile, or cyclical, standard insurance markets – in order to promote long-term stability and sufficiently reduce the ultimate cost of risk over time.
Section 3: What are the implications of using a captive for medical stop loss for the parent organization?
It should first be noted that, with the exception of group captives, it doesn't usually make sense to form a captive solely for medical stop loss. The premiums, except for very large employers, are not typically large enough to provide appropriate economic justification. The primary opportunities are for employers who already have an established captive, to which the stop loss can be added. Employers with an existing captive are likely to be self-funding medical benefits already and adding medical stop loss is an easy captive addition.
 Just as a captive is used to strategically enhance risk management efforts, adding stop loss to a captive can augment an organization's human resource reward objectives by enhancing the efficiency of employee benefit financing and delivery. One primary purpose of a captive is to provide coverage or facilitate capacity that is disproportionately expensive, or otherwise unavailable within traditional or standard insurance markets. Although some stop loss policies will provide coverage that mirrors an employer's Plan Document, most stop loss policies contain exclusions (Differences in Conditions a/k/a DICs) that conflict with the Plan Document. Stop loss carriers will also frequently identify specific individuals with large, ongoing medical conditions and exclude (a/k/a "laser") them from stop loss coverage. DICs and lasers are examples of terms and conditions that can be effectively absorbed by a captive, in order to help maintain long-term continuity to self-funded benefit delivery.
Just as a captive is used to strategically enhance risk management efforts, adding stop loss to a captive can augment an organization's human resource reward objectives by enhancing the efficiency of employee benefit financing and delivery. One primary purpose of a captive is to provide coverage or facilitate capacity that is disproportionately expensive, or otherwise unavailable within traditional or standard insurance markets. Although some stop loss policies will provide coverage that mirrors an employer's Plan Document, most stop loss policies contain exclusions (Differences in Conditions a/k/a DICs) that conflict with the Plan Document. Stop loss carriers will also frequently identify specific individuals with large, ongoing medical conditions and exclude (a/k/a "laser") them from stop loss coverage. DICs and lasers are examples of terms and conditions that can be effectively absorbed by a captive, in order to help maintain long-term continuity to self-funded benefit delivery.
Section 4: Captive Types, Explained
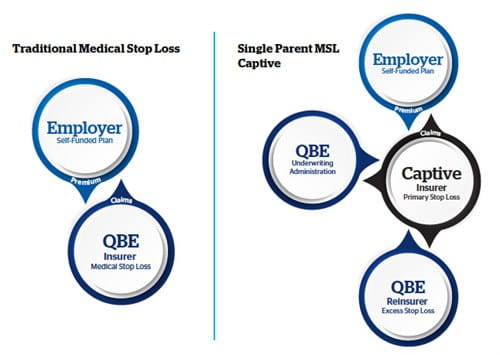
Captives for medical stop loss generally follow the same structure as the more traditional casualty captives, and both single-parent (pure) captive and group captive structures are becoming widely used.
- Single-Parent Captives: A single-parent (or pure) captive is formed as a subsidiary of another entity, referred to as the "parent" (i.e., a single owner), to insure the risks of its parent. The primary opportunities are for large individual employers who already have an established single-parent captive, to which the stop loss can be added. Many self-funded employers of this size previously did not purchase stop loss, but since the enactment of ACA and its mandate of unlimited lifetime benefit maximums within a health plan, they now purchase high (unlimited) levels of coverage and can assume some lower layers into their captive. As mentioned earlier, stop loss coverage by itself would not typically generate enough premiums to justify formation of a captive solely for that purpose. However, it can be used to effectively expand the utility and enhance the efficiency of an existing captive.
Funding layers of medical stop loss coverage through a single-parent captive, as opposed to simply paying claims within the same layers from general assets or through a formal trust, allows the employer to more easily recognize and deploy underwriting profit and investment returns attributable to these layers. Surplus derived from the underwriting and investment return from the captive can be returned to the employer (i.e., captive parent) more efficiently in the form of dividend distributions or strategically deployed to offset future plan costs, expand benefits to employees or retained within the captive to smooth financial volatility associated with other lines of coverage. Adding stop loss to a captive that primarily writes "long-tail" coverage, such as workers compensation or liability, can provide a protective "short-tail" stability hedge by diversifying the captive's risk portfolio.
- Group Captives: A group captive is a legal entity jointly owned by a group of unrelated companies, and formed primarily to insure the risk of its member-owners. There generally are two types of group captives: Heterogeneous (dissimilar industries) and Homogeneous (similar industries). The objective of both types of group captives is to enable a grouping of mid-market employers to replicate the risk profile of a single large employer to spread risk, promote stability, and achieve leveraged cost savings from different service providers.
 Heterogeneous groups generally require more participants to achieve an appropriate spread of risk among its diverse members. A larger size and risk spread are necessary to mitigate the increased risk variability, and the potential for increased underwriting volatility, caused by differing demographics among the participating employer populations. For example, the risk profile of the employee population of a 250 life professional services firm is much different than the risk profile of a 250 life construction firm. Both could be members of the same heterogeneous group captive, though size and risk spread must be appropriately proportioned to achieve sustainable stability.
Heterogeneous groups generally require more participants to achieve an appropriate spread of risk among its diverse members. A larger size and risk spread are necessary to mitigate the increased risk variability, and the potential for increased underwriting volatility, caused by differing demographics among the participating employer populations. For example, the risk profile of the employee population of a 250 life professional services firm is much different than the risk profile of a 250 life construction firm. Both could be members of the same heterogeneous group captive, though size and risk spread must be appropriately proportioned to achieve sustainable stability.
- Homogenous Groups: Being industry-specific in their composition, these groups can be smaller because their underlying risks and underwriting profiles are similar, so the size needed to achieve an appropriate spread of risk is not as large as it is with heterogeneous groups. Group captives are especially effective when formed by closely aligned groups (or associations) of like-minded employers within the same industry. Risk Retention Groups (RRGs) are a form of homogenous group captives. RRGs are only authorized by the Federal Liability Risk Retention Act (LRRA) to cover liability risks; however, the potential exists for groups of employers participating in RRGs to form a parallel group captive for medical stop loss coverage. The average individual member size within homogeneous groups also tends to be larger than it is in heterogeneous groups and, given the similarity of the participants' employee populations, an appropriate risk spread can be achieved within a smaller group of employers
- Open-Market Groups: There is a sub-category of group captives that we generally refer to as open-market group captives. These captives are typically heterogeneous programs sponsored by large brokers, captive managers, or other program administrators. They are
 "open" to new members who meet the eligibility guidelines established for entry. The average member size within this category is typically smaller than in other group captives, and is generally between 50 and 250 employees (lives). It is important to note that smaller employers have less underwriting credibility, and tend to be more unpredictable within this range. Given the smaller average member size and differing risk demographics, it is especially important for open-market heterogeneous captives to achieve both the size and appropriate risk spread that will enable them to hedge volatility.
"open" to new members who meet the eligibility guidelines established for entry. The average member size within this category is typically smaller than in other group captives, and is generally between 50 and 250 employees (lives). It is important to note that smaller employers have less underwriting credibility, and tend to be more unpredictable within this range. Given the smaller average member size and differing risk demographics, it is especially important for open-market heterogeneous captives to achieve both the size and appropriate risk spread that will enable them to hedge volatility.
Group captives can be structured as traditional member-owned captives or as rent-a-captives (RACs). A RAC is a captive insurance company owned by a nonaffiliated sponsoring entity, typically an insurance company, which "rents" space within the pre-established captive to insureds. This rental structure provides many of the same benefits, without much of the required financial commitment associated with traditional (member-owned) captives. RACs may also be structured as segregated (or protected) cell companies in which the assets and liabilities of each group of participants are legally separated from other groups, and cannot be used by other members to meet their liabilities.
Section 5: Are group stop loss captives considered MEWAs?
Group captives are not considered Multiple Employer Welfare Associations (MEWAs), and that is an important distinction. In a MEWA, premium contributions from several employers are commingled into a single trust or custodial account, and used either to purchase insurance or pay claims directly to providers or employees. All MEWA funds are controlled and managed by a centralized administrator, leaving room for little or no control by employers.  MEWAs are also heavily regulated by the few states that actually permit them.
MEWAs are also heavily regulated by the few states that actually permit them.
In a group stop loss captive, each employer establishes a separate self-funded benefit plan and purchases a separate medical stop loss policy. There is no comingling of plan assets, nor is there joint risk sharing among the benefit plans of individual participating employers. Each employer maintains full control of their benefit plan, including the ability to set funding levels, and select, appoint, and control plan administrators, TPAs, and most other related service components. The captive participates only in the medical stop loss coverage, which is separate, and not directly connected, to the benefit plan itself.
Section 6: Mechanics of a Group Captive
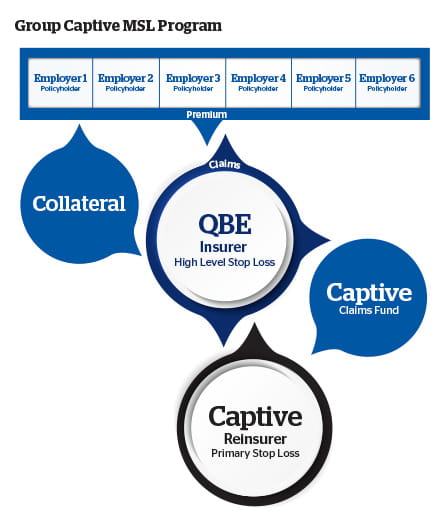
Within a group captive, each employer establishes a separate self-funded plan for their own employees, and purchases medical stop-loss coverage according to their own risk appetite. The stop-loss is purchased from the common insurer or reinsurer that will provide coverage to each member of the captive. The actual captive participation level will be determined by the collective risk appetite of the insured members, and can be structured on either an excess or quota-share participation basis.
The basic structure of a stop-loss captive is fairly simple:
- The group participants select a common stop-loss insurer to provide coverage to all members.
- Once a viable participation commitment (critical mass) has been achieved, each member will establish and maintain an individual self-funded healthcare plan. This will include choosing the desired plan design and all related service components, such as third-party administrators (TPAs), provider networks, and the like. Although each member's plan is designed and maintained separately, the size advantages of the group can be leveraged, if related components are collectively obtained from common providers.
- Each member purchases specific and aggregate medical stop-loss coverage, according to their own risk appetite. The stop loss is purchased from the common insurer or reinsurer that will provide coverage to each member of the captive.
- The stop-loss carrier then cedes a portion of the collective stop-loss portfolio, attributable to all participating group members, to a captive owned jointly by all participating members. (For example, the captive would assume risk participation within the $250,000 excess of $250,000 layer or $500,000 excess of $500,000 layer within the collective portfolio.) The actual captive participation level will be determined by the collective risk appetite of the insured members, with agreement from the ceding carrier.
Group captives can increase leverage with carriers, provider networks, and related service providers, in order to generate volume-related discounting that typically would not be within reach of many individual self-insurers. By retaining an additional participation layer through the captive, the pricing volatility associated with the stop-loss coverage can be mitigated.
 Employers with more than 1,000 employee lives typically have little mechanical or financial difficulty in maintaining a self-funded program, and have access to stop-loss coverage in relative abundance. Medical stop-loss and overall structural options for smaller and mid-sized companies (those having between 100 and 500 employee lives) can be more challenging. Group captives show significant promise in enhancing self-funded program stability, and in expanding the accessibility of stop-loss to employers within this segment. Group captives are not new; they have been effectively used to cover the casualty exposures of mid-sized employers for decades.
Employers with more than 1,000 employee lives typically have little mechanical or financial difficulty in maintaining a self-funded program, and have access to stop-loss coverage in relative abundance. Medical stop-loss and overall structural options for smaller and mid-sized companies (those having between 100 and 500 employee lives) can be more challenging. Group captives show significant promise in enhancing self-funded program stability, and in expanding the accessibility of stop-loss to employers within this segment. Group captives are not new; they have been effectively used to cover the casualty exposures of mid-sized employers for decades.
Both single-parent and group captives are empowered with the control to select unbundled service providers, determine coverage levels, manage losses, direct the use of surplus, and, ultimately, share in the results – ideally generating a bottom-line profit. Effectively exercising these capabilities helps firms strategically reduce the cost of risk while optimizing their long-term stability.
Section 7: How to Determine Whether a Stop Loss Captive Is Appropriate for an Employer
Whether or not to make use of a stop loss captive is a collaborative process, one involving the client and their consultant/broker, along with the (re)insurance carrier. Client suitability for captive participation is predicated upon their financial management and employee benefit objectives, followed by the selection of the most efficient structure to achieve those objectives. Self-funding is based on retaining predictable segments of risk, while transferring the more unpredictable risk layers to an insurer. The level of appropriateness for participation in a captive is determined by an employer's ability to assume additional risk, along with a slight increase in administrative responsibility, in order to achieve an enhanced reduction in overall plan costs.
In terms of appropriate characteristics, size is the first consideration. Can the entity efficiently (and perhaps sufficiently) assume enough credibly predictable risk to achieve a commensurate return? For single-parent captives, assuming the owner is adding stop loss to an existing captive, $1 million of premium is a normal benchmark for minimum appropriateness. For group captives, the minimum threshold is generally 10 employer groups, or 1000 lives (averaging 100 lives each), and $2.5 million of premium, with a more homogenous (industry-specific) member composition being preferable, from an underwriting standpoint. As mentioned earlier, the more heterogeneous the group, the larger it needs to be, in order to attain an appropriate spread of risk across various industry classifications and employer sizes.
Whether single-parent or group captive, all employers must demonstrate the following: appropriate financial stability, a willingness to assume risk, and a commitment to sound risk management and the promotion of improved employee health and wellness.
Section 8: Department of Labor, ERISA, and State Regulation
For stop loss captives, it is important to differentiate self-funding and medical stop-loss insurance from the healthcare insurance plan itself. This distinction is important because the captive is a separate entity, unconnected to the actual benefit plan (The Plan) provided to employees. The U.S. Department of Labor (DOL), by way of the Employee Retirement Income Security Act (ERISA), has regulatory jurisdiction over the plan itself, but does not regulate insurance. Within a self-insured structure, the employer assumes the financial liability for all the claim obligations of the plan. Medical stop-loss coverage, purchased by the plan sponsor, does not insure the plan; rather, it indemnifies the sponsor for its claim obligations to the plan. In this regard, the DOL only regulates a plan sponsor's responsibilities as they relate to overall plan administration, and the delivery of benefits to employees. Individual states regulate insurance, including medical stop loss. However, since the plan is self-insured (and specifically deemed by ERISA not to be insurance), state insurance mandates are preempted, and are therefore not applicable in relation to the plan.
Section 9: Does a stop loss captive require DOL approval?
Any employee benefit insurance (other than voluntary coverages) that provides coverage directly to an employee will require an ERISA Prohibited Transaction Exemption (PTE) from the DOL, for inclusion into a captive. Since the self-funded medical plan itself is not part of the captive, it does not require a PTE.  Medical stop loss is not recognized by the IRS as a plan asset and, as mentioned previously, it insures the employer rather than the employer's employees. It is not considered employee benefit coverage, and since neither the DOL nor ERISA have regulatory jurisdiction, a Prohibited Transaction Exemption (PTE) is not applicable to a medical stop-loss captive, and is not required from the DOL. The fact that medical stop loss insurance is not considered employee benefit coverage was recently affirmed by the U.S. DOL in a November, 2014 technical release (US DOL No. 2014-01).
Medical stop loss is not recognized by the IRS as a plan asset and, as mentioned previously, it insures the employer rather than the employer's employees. It is not considered employee benefit coverage, and since neither the DOL nor ERISA have regulatory jurisdiction, a Prohibited Transaction Exemption (PTE) is not applicable to a medical stop-loss captive, and is not required from the DOL. The fact that medical stop loss insurance is not considered employee benefit coverage was recently affirmed by the U.S. DOL in a November, 2014 technical release (US DOL No. 2014-01).
Section 10: Fronted Insurance versus Reinsurance
Since medical stop loss is not a statutorily mandated coverage, single-parent captives do not usually need to be "fronted" by an insurance company. The captive itself is recognized as an insurance company by its domicile, and can issue a stop loss policy to its own parent, i.e., the employer. For this reason, medical stop loss coverage for a single-parent captive can be provided in the form of reinsurance rather than insurance. As reinsurance, much of the expense associated with the issuance of an insurance policy (front fees, premium taxes, collateralization, and so forth) has been stripped out, thus reducing the cost of coverage. Being able to write stop loss as a reinsurance transaction is usually the most efficient structure for single-parent captives, which in most cases will not require a fronting carrier.
Group captives will normally be required to have an authorized carrier issue an approved stop loss policy to its member-owners. In most cases, captive insurance companies are recognized as "non-authorized" insurers by the National Association of Insurance Commissioners (NAIC) and by states. Since stop loss insurance is regulated by the states, most will require that any entity acting as an insurance company must be recognized as an authorized insurer, and appropriately licensed by the individual state(s), in order to issue an insurance policy to non-affiliated entities, i.e., group members. Therefore, most group captives are typically structured behind a front company, which issues a stop loss policy, and then cedes risk to the captive as a reinsurer.
Ceding insurance to a captive, behind a front, obviously adds to the captive's expense structure, and because the captive itself is not recognized by the NAIC as an "authorized reinsurer," some level of collateralization, commensurate with the amount of risk ceded to the captive, will be required. However, most of these expenses would be part of a traditional self-funded program, and are offset by the potential underwriting and investment returns generated by the captive, and returned as dividends or premium credits to the owner-members.
Section 11: Does medical stop loss enhance the tax advantages of a captive?
There are differing opinions about the answer to this question. Even though medical stop loss can provide beneficial risk portfolio diversification for a captive, our opinion is that it should not be considered third-party risk, for single-parent captive tax purposes. It is generally recognized that captives generating some degree of premium (50% is considered a safe harbor) from unrelated, or third-party, risk, may be able to claim premium deductions. Employee benefit insurance coverage that pays benefits directly to the employee, or to healthcare providers on behalf of the covered person,  is recognized as third-party captive risk by the Internal Revenue Service. However, because medical stop loss insurance provides coverage to the employer, rather than directly to employees, no third-party risk exists. The distinguishing element is determined by whose liabilities are actually being insured – the employer's or the employee's. This interpretation was reaffirmed by the U.S. DOL in the previously mentioned 2014 technical release. Taxation circumstances for group captives may be different, however, as the participating member-owners are unrelated entities. Since we are unable to provide tax advice, and as there have been some conflicting opinions, our recommendation is to always seek appropriate guidance from a qualified captive tax attorney.
is recognized as third-party captive risk by the Internal Revenue Service. However, because medical stop loss insurance provides coverage to the employer, rather than directly to employees, no third-party risk exists. The distinguishing element is determined by whose liabilities are actually being insured – the employer's or the employee's. This interpretation was reaffirmed by the U.S. DOL in the previously mentioned 2014 technical release. Taxation circumstances for group captives may be different, however, as the participating member-owners are unrelated entities. Since we are unable to provide tax advice, and as there have been some conflicting opinions, our recommendation is to always seek appropriate guidance from a qualified captive tax attorney.
Section 12: Risk Management Critical to Success
Just as self-insured casualty programs utilize loss control techniques to improve employee safety and mitigate claims, it is imperative for self-insured health care plans to employ effective cost containment measures. Programs such as utilization review, large case management, and negotiated provider discounts, have long-proven their effectiveness for reducing the cost of claims, after they occur. Newer initiatives, such as employee wellness programs and predictive modeling, strive to preemptively reduce claim expenses by improving the overall health of the employee population. Increasing employee wellness will help to significantly decrease the cost of providing employee health care coverage – not immediately, but over time, as the effects of the wellness program matriculate. More progressive plans incorporate elements such as referenced-based pricing, virtual (telemedicine) care, and medical tourism into their design, as additional cost-reduction techniques. There will be some increase in fixed costs associated with the implementation of some risk management initiatives; however, the savings generated by the corollary reduction in claims costs – a much larger expense – will offset the initial expenses, over time.
Section 13: Domicile Considerations
Unlike captives that provide employee benefits requiring a DOL PTE, a medical stop loss captive is not required to be domiciled onshore. Since more offshore captives have made the IRS 953(d) election to be taxed as a U.S.-based corporation, the advantages of incorporating offshore have eroded. In reality, most single-parent stop loss coverage will be added to an existing captive, so the domicile decision becomes automatic. In most cases, the existing domicile will only require an expansion or amendment to the original captive business plan, while ensuring that the appropriate surplus has been established to accommodate the new line of business.
Domicile selection for group captives is a bit different. More of these are being established solely to write stop loss, and as such, the incorporations have gravitated to domiciles that are friendlier to, and familiar with, the nuances specific to group captives, such as the Cayman Islands, Bermuda, and Vermont.
Conclusion: Continued Growth Expectations
Interest in self-funding and stop loss captives will continue to grow as medical costs continue to rise, and uncertainties related to the ACA threatens the amount of control employers can maintain within more conventional insurance structures. Properly structured captives can stabilize, and even lower the cost of medical stop loss coverage, and they can facilitate enhanced benefit delivery, over more traditional self-insurance, for many employers.
The QBE Solution QBE's North American-based Accident & Health Division provides exemplary coverage and services to support the specialized needs of self-insured employers as a leading direct-writing provider of medical stop loss, including single parent and group captive programs requiring stop-loss insurance.
About QBE North America QBE North America is part of QBE Insurance Group Limited, one of the largest insurers and reinsurers worldwide. QBE NA reported Gross Written Premiums in 2015 of $4.6 billion. QBE Insurance Group's 2015 results can be found at qbe.com/us. Headquartered in Sydney, Australia, QBE operates out of 43 countries around the globe, with a presence in every key insurance market. The North America division, headquartered in New York, conducts business through its property and casualty insurance subsidiaries. QBE insurance companies are rated "A" (Excellent) by A.M. Best and "A+" by Standard & Poor's.* Additional information can be found at qbe.com/us, or follow @QBENorthAmerica on Twitter.